 DE
DE FR
FR IT
IT ES
ES

Genital herpes
Genital herpes is the most common sexually transmitted ulcer disease in developed countries. It is caused by human herpesviruses type 1 (HSV-1) or 2 (HSV-2), 2 of the 8 types of herpesviruses infecting humans.
After initial infection, the herpes simplex virus remains latent in the nerve ganglia, from where it can periodically reactivate. This reactivation can be asymptomatic or cause symptoms (in this case, genital lesions). Transmission occurs through contact with the lesion or, more commonly, through close body contact with a sexual partner when the damage is not obvious (called asymptomatic spread).
Pregnant women with genital herpes can transmit HSV (usually HSV-2) to their fetus or newborn; HSV is usually transmitted during childbirth through contact with vaginal secretions that contain HSV. Transplacentally, the virus is rarely transmitted. Mothers with primary (recently acquired) genital HSV infection have a higher risk of transmitting the virus to their newborn. Most women who contract HSV in their newborns do not have symptoms of HSV infection during childbirth. HSV infection in newborns is a serious, potentially fatal infection.
Clinical manifestations
Most cases of primary genital herpes do not cause noticeable symptoms; many people infected with HSV-2 are unaware that they have genital herpes.
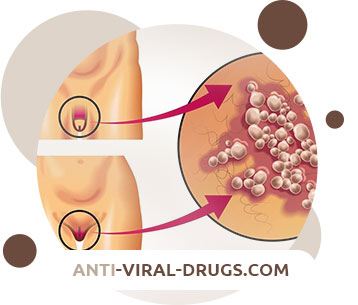
Primary genital lesions develop 4–7 days after exposure. The blisters usually rupture and form ulcers that can coalesce. Lesions can occur in the following places:
- On the foreskin, head and body of the penis in men
- On the labia, clitoris, perineum, vagina and cervix in women
- Around the anus and rectum of men or women who have receptive anal sex
Urinary hesitancy, dysuria, urinary retention, constipation, or severe sacral neuralgia may develop.
Scars may remain after healing. Relapses occur in 80% of HSV-2 patients and 50% of HSV-1 patients.
Primary genital lesions are generally more painful, prolonged, and extensive, and are more likely to be bilateral and involve regional adenopathy and constitutional symptoms than recurrent genital lesions. Relapses of the disease tend to be milder and present with fewer symptoms.
Diagnostics
- Clinical evaluation
- Inoculation for culture and polymerase chain reaction (PCR)
- Serological testing
Genital herpes is often diagnosed based on the presence of characteristic lesions; groups of vesicles or ulcers on an erythematous basis are uncommon for genital ulcers, except for those caused by the herpes simplex virus. However, these lesions are absent in many patients.
If the diagnosis is unclear, tests to detect HSV are necessary.
The examination usually involves taking a sample of fluid from the base of the vesicle or from a recent lesion, if present. The absence of HSV during cultivation, especially in patients without active lesions, does not exclude HSV infection, since the release of the virus is not constant. In addition, the virological method has limited sensitivity; PCR is more sensitive and used more frequently.
Direct immunofluorescence with labeled monoclonal antibodies is sometimes available; this method is highly specific but not very sensitive.
Serological tests are able to detect with great accuracy antibodies to HSV-1 and HSV-2, which develop during the first few weeks after infection and are then constantly present in the body. Thus, if infection with genital herpes is believed to be recent, the tests may need to be repeated to allow time for seroconversion to occur.
Serologic tests for HSV have several purposes:
- Evaluation of patients who do not have suspicious genital lesions, but who need this examination or want to undergo it themselves (for example, due to past genital lesions or high risk behavior)
- To help determine the risk of developing focal lesions
- Identifying pregnant women who do not have genital lesions but are at risk of transmitting herpes to their newborn during labor
- Determining the risk of contracting a healthy partner from a sexual partner with an existing genital herpes
Treatment
- Acyclovir, valacyclovir, or famciclovir
Genital herpes is treated with antiviral drugs.
Primary eruptions are treated in one of the following ways:
- Acyclovir 400 mg orally 3 times a day for 7-10 days
- Valacyclovir 1 g orally every 12 hours for 7-10 days
- Famciclovir 250 mg orally 3 times a day for 7-10 days
These drugs reduce the spread of the virus and the symptoms of severe primary infections. However, even early treatment of primary infections does not prevent recurrence.
With repeated rashes, the duration and severity of symptoms may be slightly reduced by antiviral treatment, especially during the prodromal phase. Recurrent rashes are treated in one of the following ways:
- Acyclovir 400 mg orally 3 times a day for 5 days
- Valacyclovir 500 mg orally every 12 hours for 3 days
- Famciclovir 1000 mg orally every 12 hours for 1 day
For frequent rashes (eg,> 6 rashes / year), suppressive antiviral therapy with one of the following:
- Acyclovir 400 mg orally every 12 hours
- Valacyclovir 500 to 1000 mg orally once a day
- Famciclovir 250 mg orally every 12 hours
Doses should be adjusted according to renal function. Adverse effects are uncommon when taken orally, but may include nausea, vomiting, diarrhea, headache, and rash.
Topical antiviral drugs are of only minor importance and their use is not recommended.
Evaluation of the sexual partners of patients with genital herpes is important.

Prevention
The best ways to avoid genital herpes are
- Abstaining from sexual contact (vaginal, anal and oral sex)
- Long-term mutually monogamous relationship with a trusted and uninfected partner
The risk of genital herpes can be reduced by
- Correct and consistent use of latex condoms
However, condoms are not able to isolate all areas of the body where contact with the virus can occur, and thus cannot fully protect against genital herpes.
Patients with genital herpes should refrain from sexual activity if they have lesions or other symptoms of herpes. Patients should be reminded that they can transmit infection even if they do not have any symptoms.
Prevention of neonatal herpes infection
Efforts to prevent neonatal transmission of the virus have not been very effective. Universal screening has also proven ineffective or is not recommended.
Doctors need to ask all pregnant women if they have had genital herpes before and emphasize the importance of avoiding infection during pregnancy.
If a woman has symptoms of herpes (such as active genital lesions), a caesarean section is recommended to prevent transmission of the virus to the newborn. Pregnant women with genital herpes can be given acyclovir starting at 36 weeks gestation to reduce the risk of recurrence and therefore the need for a caesarean section.
During labor, the head should not be assessed if the mother is suspected of having an active genital herpes.





